
From the 1Department of Health Sciences, Lund University, 2Department of Neurology and Rehabilitation Medicine, Skåne University Hospital, Lund, 3Department of Health Science, Luleå University of Technology, Luleå, 4The PRO-CARE Group, School of Health and Society, Kristianstad University, Kristianstad, Sweden
Objective: To explore how persons with late effects of polio experience falls and what strategies they use to manage the consequences of falls.
Design: A qualitative study with face-to-face interviews. Data were analysed by systematic text condensation.
Participants: Fourteen ambulatory persons (7 women; mean age 70 years) with late effects of polio.
Results: Analysis resulted in one main theme, “Everyday life is a challenge to avoid the consequences of falls”, and 3 categories with 7 subcategories. Participants perceived that falls were unpredictable and could occur anywhere. Even slightly uneven surfaces could cause a fall, and increased impairments following late effects of polio led to reduced movement control and an inability to adjust balance quickly. Physical injuries were described after the falls, as well as emotional and psychological reactions, such as embarrassment, frustration and fear of falling. Assistive devices, careful planning and strategic thinking were strategies to prevent falls, together with adaptation and social comparisons to mitigate the emotional reactions.
Conclusion: Experiences of falls greatly affect persons with late effects of polio in daily life. To reduce falls and fall-related consequences both problem-focused and emotion-focused strategies are used. In order to increase daily functioning, these findings should be included in a multifaceted falls management programme.
Key words: activities of daily living; coping skills, accidental falls; emotions; post-poliomyelitis syndrome; qualitative research.
Accepted Jun 15, 2017; Epub ahead of print Aug 9, 2017
J Rehabil Med 2017; 49: 00–00
Correspondence address: Christina Brogårdh, Physiotherapy Research Group, Department of Health Sciences, Box 157, Lund University, SE-221 00 Lund, Sweden. E-mail: christina.brogardh@med.lu.se
Persons ageing with late effects of polio (LEoP) are at high risk of falls (1). New or increased impairments that often occur several decades after an acute poliomyelitis infection can lead to ambulation difficulties and thereby increase the risk of falls (1, 2). Up to 80% of persons ageing with LEoP report at least one fall per year (1, 3–9), which is 2–3 times higher than in non-disabled elderly persons (10), but comparable to persons with other neurological disabilities (11–13).
Studies have shown that most falls in persons with LEoP occur in the afternoon and outdoors during activities related to walking (1, 5, 9). Bruises and sprains are the most common injuries, but some persons also sustain fractures (1, 3, 5, 14). Factors associated with falls are discrepancies in leg length (9), muscle weakness in the lower limbs (5, 8, 15), reduced balance (5, 15), walking limitations (1, 8), and fear of falling (5), which may decrease life satisfaction (16).
Despite the fact that falls are very common in persons with LEoP, there have been no studies from the individual’s perspective of how these experiences impact on daily life. Previous studies have used pre-defined questionnaires, which may limit a detailed understanding of the phenomenon. Experiences of falls and fall-related consequences have been described in persons with stroke (17), spinal cord injury (SCI) (18) and multiple sclerosis (MS) (19). In these studies the participants expressed fear of injuring themselves due to a fall, fear of not being able to get up after falls, and increased limitations in many daily situations. Persons with LEoP may have similar experiences, but there is currently very limited knowledge. In order to provide appropriate rehabilitative support to persons with LEoP there is a need for a more in-depth understanding of how they experience the circumstances around their falls, reactions and consequences for daily life, as well as strategies to overcome perceived adversities. The aim of this qualitative study was therefore to explore how persons with LEoP experience falls and what strategies they use to manage the consequences of falls.
This qualitative study is based on semi-structured face-to-face interviews. Data were analysed by systematic text condensation (20), which is a descriptive and explorative method inspired by phenomenological theory. This method is suggested for use when developing new descriptions and concepts from multiple informants.
Participants with a confirmed history of acute poliomyelitis and with new impairments after a period of functional stability were recruited from a post-polio rehabilitation clinic in southern Sweden. The participants had previously taken part in another study of falls (1). From that cohort a wide range of variations were sought by strategically selecting participants of different sex, age, functional level, years with LEoP, and fall frequency (21).
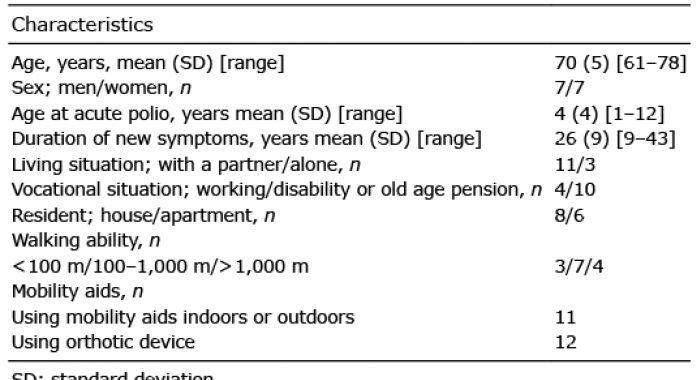
Eighteen persons were contacted by telephone and informed about the study, and 14 (7 men) agreed to participate (Table I). Their mean age was 70 years, mean age at the acute poliomyelitis infection was 4 years, and mean duration of new symptoms of LEoP was 26 years. Most participants lived with a partner and were in receipt of part-time disability pension or old-age pension. All were able to walk at least 100 m, and the majority used a stick and/or orthotic device during ambulation.
Table I. Characteristics of the 14 participants with late effects of polio
All persons received oral and written information prior to the study and gave their informed consent to participate. The principles of the Declaration of Helsinki were followed, and the study was approved by the Regional Ethical Review Board, Lund, Sweden (Dnr: 2014/186).
This study was part of a larger project on ageing with LEoP. The interviews were conducted at the post-polio rehabilitation clinic by 2 of the authors (CB, CSH), and lasted between 60 and 90 min. The interviewers have professional experience of persons with LEoP, but had no therapeutic relationship with the participants. During data collection an interview guide was used that included open-ended questions about: (i) experiences of falls; (ii) circumstances around the falls; (iii) consequences of the falls; (iv) strategies to prevent falls and to overcome adversities. Follow-up questions, such as: “Can you give an example?” and “Please, describe”, were used. All interviews were recorded and transcribed verbatim.
Data analysis was completed in the following 6 steps:
The latent analysis resulted in 1 main theme: “Everyday life is a challenge to avoid the consequences of falls” and 3 categories based on 7 subcategories: “Falls can occur anywhere”; “Physical and psychological consequences of the falls”; and “A variety of strategies to reduce falls and the fall-related consequences” (Fig. 1).
Fig. 1. The main theme with the 3 categories and 7 subcategories that emerged from the latent analysis.
The participants perceived that falls were difficult to foresee and could occur anywhere. Even slightly uneven surfaces could cause a fall and their increased impairments following LEoP led to reduced movement control and an inability to adjust balance quickly.
Impairments lead to unpredictable falls. The increased impairments following LEoP, such as muscle weakness in the more affected limb, led to an inability to lift and control the limb. The leg could suddenly give way and the forefoot was easily hampered by unevenness of the floor, which caused unpredictable falls. Many perceived a reduced body control and a feeling of un-steadiness, but were unable to adjust balance quickly. Difficulties in concentrating on mobility, especially when in a hurry, were also perceived as problematic and increased the risk of falls.
No, I don’t have time to adjust. Sometimes you feel that the foot doesn’t really “keep up” and then you fall or you try to find the balance again. It happens quite often. (Participant 1; P1)
In any situation the legs simply give way, so the falls can occur at any time. (P4)
Falls occur in many different places. Falls were equally common indoors and outdoors, and occurred in many different places. One risky place indoors was the bathroom, where the falls typically occurred when taking a shower and standing on 1 leg to wash the feet. Other common fall situations indoors were stumbling over carpets, when starting to walk after getting up from an armchair, and when entering a lift or climbing stairs.
If I’m taking a shower… I don’t dare to stand up, I’ve fallen and it almost ended dreadfully… (P12)
Falls also easily took place outdoors, for example when walking on a lawn, gravel paths or on cobblestones, but also when stepping up onto pavements without a walking aid or walking on slopes or wet surfaces. Slightly uneven or slippery surfaces could cause a fall and participants were often astonished how a fall could happen.
It’s when I’m walking outside. Suddenly you just lie there on the ground. But sure enough, if you look down there was some uneven surface, but not that much that I would expect it to be enough to trip over and fall. (P1)
I was just spinning around, if I had… was going out to water the flowers… I don’t know what I did, if two blades of grass were in the way, I don’t know. (laughter) I just fell and sprained my ankle and twisted my leg. (P7)
Public places, e.g. at shopping malls when pushing shopping trolleys, or train stations on account of marble-surfaced floors were other locations where falls typically occurred. In the winter, falls also occurred outside shops due to high banks due to snow clearance.
I fell at the station… and it could have gone completely wrong. There was a marble floor and I slipped, I fell flat. Those are things you have to think about. (P12)
A variety of fall-related consequences was described among the participants, and comprised physical injuries, but also emotional and psychological reactions after the falls.
Physical injuries. Some of the participants had experienced milder injuries, such as bruises and skin sores. Others had been more severely injured, often several times, and they mentioned injuries to the knees, teeth and jaws, fractures of the arms, legs, ribs, spine, but also head trauma with concussions that required hospital care.
I hit a painted concrete floor and I hit, well, I flew a couple of meters ahead I think… I hit my mouth and forehead and… one tooth was knocked out. (P7)
Emotional and psychological reactions. Many described varying degrees of emotional and psychological reactions after the falls. Some felt embarrassed when falling outdoors and felt a need to immediately look around to see if anybody had noticed it. Others felt angry and frustrated, and were afraid that they had been injured. Some described that they occasionally felt stupid when falling, but that it did not bother them too much. On the other hand, there were those who feared that other persons who had observed the fall might believe that they were not sober.
I mean you’re always scared right when you’ve fallen, before you’ve checked. Oh, am I unharmed and clean? Okay, then it’s fine to get up. (laughter) (P13)
…falling in town I mean, then, people might think that you’re not sober. (P7)
A fear of falling was described by most of the participants, but to varying degrees. Falling indoors was generally perceived as less frightening than outdoors, as there was often furniture to grab. Walking and carrying things at the same time, for example a tray or a grandchild, were situations that caused many to feel insecure. Going downstairs or getting in and out of escalators was also perceived as problematic, as the leg easily might give way. Some described that they were afraid of being injured after the falls, whereas a few participants said that they were so used to the risk of falling that they were no longer afraid.
…I have a little grandchild of 9 months old, but I don’t dare to walk and carry him around at the same time. I didn’t dare that with my older grandchild either when she was little. There I feel a fear, “what if I fall”. (P 6)
The fear of falling also influenced the ability to perform leisure activities, for example swimming, climbing up a ladder, or walking in the woods. Some perceived cycling to be problematic, to get over an obstacle and not being able to put the foot down quickly enough to maintain balance. Many were worried about walking outdoors during slippery conditions and 1 participant even reported having anxiety attacks with just the thought of walking outside when the temperature had dropped.
As soon as autumn comes or something, I know it’s plus ten degrees, it hasn’t snowed, nothing has frozen. But it’s wet and looks glossy, then… I can’t take a step. (P13)
Some of the participants were particularly afraid of falling outdoors as they needed external support to get up. One man described how he had to cross the street on his hands and knees to reach something to grab, in order to be able to pull himself up.
What you’re afraid of, if you’re alone in an urban environment, is falling where there’s nothing to grab. Then you have to crawl to something… you feel uncomfortable walking in places where you don’t find anything to grab. (P4)
A variety of strategies to reduce falls and the fall-related consequences
Various strategies were used by the participants to reduce falls and the fall-related consequences. They mentioned the importance of using assistive devices, careful planning and strategic thinking, which included avoiding activities that were perceived too difficult or risky to perform. Comparing oneself with others or adapting to their changed capability were other common strategies to mitigate the emotional and psychological reactions of falls.
Using aids to prevent falls. A variety of aids, such as banisters, chairs and non-slip mats for baths and showers, a night lamp for a brighter view and different types of mobility aids, shoes and orthoses, depending on the surface, were used to prevent falls. However, using a mobility aid was also perceived as risky, as it limited the ability to protect oneself if falling; therefore some used a backpack to increase safety when walking. Other strategies were using Nordic walkers or spikes on the shoes or on the cane when it was slippery or icy outdoors.
…If I’m carrying something I also use a backpack. I feel like if you have one arm that’s locked to a crutch or a cane you don’t really feel safe. If something were to happen, you really want to be able to protect yourself with your hands and then I’ll have at least one hand free. (P5)
I have to think about where I’m going and during winter I have to have some kind of support with me, for example my Nordic walkers. If it’s really slippery, I also use spikes, they work well. (P3)
Careful planning and strategic thinking. Careful planning and strategic thinking were other strategies that the participants mentioned to prevent falls. They described how they had to plan every action in advance; for example, removing carpets and thresholds, using furniture and walls as support, standing still in darkness or after getting up from a chair to regain balance, and being extra cautious and attentive in the bathroom.
… if I’m getting up I support myself on a table and then I keep still in order regain balance to stay upright. Likewise the way you act in the bathroom, you have to think a little bit differently from a non-disabled person. I guess it’s about that. (P12)
Other strategies were waiting until the pavement was gritted before going out, or walking on different paths where the surface was less uneven and slippery, but also softer, in case a fall occurred. Some participants also walked more slowly and looked down at the ground to avoid potential hazards. Another strategy was to take plenty of time and to rest when feeling tired.
I think more about it now. If I’m very tired one day or very tired in my legs, then I always think about walking carefully so I don’t fall. (P1)
Avoiding activities that were perceived as too difficult or risky to perform was another strategy. Many avoided climbing up and down stools and ladders, cutting the grass, carrying things when walking, but also avoided walking in the woods and on non-sanded pathways. However, 1 participant said that even though he tried to avoid situations that usually caused falls, he nevertheless fell.
Well, you try to avoid situations where you may fall… you know the situations when you usually fall, and then you try to avoid them. For example, when it’s slippery, there’s no winter, a week after it’s started snowing I’ve probably fallen, that’s for sure, even though you’re so careful. (P10)
Adaptation and social comparisons. Strategies to mitigate the emotional and psychological reactions related to the falls were adaption to the changed condition following LEoP, but also to compare one’s capability with other elderly non-disabled persons. Many had learned to live with their disability and therefore acted more carefully when performing activities of daily living.
I can’t walk around and be scared. But still, there’s a warning bell somewhere. Since I’ve lived with this condition all my life, I’ve gradually had to adapt to changes. It’s like that for everyone in life, but maybe a little more for “us”. (P5)
To the best of our knowledge, this is the first qualitative study to explore how persons with LEoP experience falls and what strategies they use to manage the consequences of falls. Overall, the participants perceived that falls were unpredictable. Their increased impairments following LEoP led to reduced movement control and an inability to adjust balance quickly, which made them vulnerable to slightly uneven or slippery surfaces. Physical injuries were common after the falls, as were emotional and psychological reactions. To prevent falls assistive devices, careful planning and strategic thinking were used, but also adaptation and social comparisons to mitigate the emotional reactions.
The participants experienced that the falls were difficult to predict and could occur anywhere. Often falls were caused by a combination of environmental barriers and the disability following LEoP. Our findings that falls could happen at any time and in different environments differ somewhat from previous quantitative studies in persons with LEoP (1, 5, 9), which have reported that falls mostly occur outdoors and in the afternoon. In the present study, falls were reported to occur equally often indoors and outdoors, mostly during personal daily activities or during leisure activities that required a high degree of postural control and walking ability.
It has been shown that reduced muscle strength in the lower limbs (5, 8, 9), decreased postural control (5, 8, 15), leg-length discrepancies (9) and walking limitations (1, 8) are associated with falls in persons with LEoP. However, this qualitative study has provided a deeper understanding of how impairments following LEoP can affect movement control and walking ability, which makes people more vulnerable to barriers in different surroundings and to seasonal changes. All participants were influenced by the climate; slippery or icy ground made it difficult to walk outdoors, which often forced participants to be very cautious and sometimes to stay at home. Similar experiences of how impairments, walking limitations and environmental barriers increase the risk of falls and lead to activity limitations and participation restrictions have also been described in elderly persons (22) and in persons with other neurological disabilities (17–19, 23). Thus, to increase participation for persons with disabilities it is of great importance to make the environment more accessible, not only through housing adaptations, but also through urban planning, snow clearance and adjustments to walking paths.
The participants’ narratives about the consequences of falls were multifaceted and included not only physical injuries, but also emotional and psychological reactions. Some described minor physical injuries after their falls, but many had also experienced more serious injuries that required hospital care, which is in line with previous quantitative studies in LEoP (1, 5). The emotional reactions, e.g. feeling embarrassed when falling, worried that other people would think they were not sober, fear of hurting themselves and not being able to get up on their own, have not been described previously in persons with LEoP. However, similar experiences of feeling embarrassed, being observed and judged by others have been described in elderly subjects (24) and in persons with other neurological conditions (17–19).
Many participants in the present study expressed a fear of falling and, for some, the fear was constantly in their mind. This fear intruded on many daily activities and hindered them from performing household activities, recreational and leisure activities, and participating in social events. Similar consequences of fear of falling are described in persons with MS (19), stroke (17) and SCI (18). Previous studies of persons with LEoP have used different versions of the Falls Efficacy Scale (1, 5, 8, 25) to assess fear of falling, and have reported that fear seems to be greatest in activities related to walking. It was also evident here that fear of falling was common during ambulation. However, qualitative interviews allowed the participants to give a richer description of other situations when fear of falling occurred, which increases the understanding of the phenomenon. Thus, to increase functioning in persons with LEoP, not only the physical consequences, but also emotional reactions after falls, should be considered during rehabilitation.
To reduce falls and the consequences of falls, participants used a variety of strategies, both active practical coping strategies (i.e. problem-focused) and more passive emotion-focused coping strategies (i.e. avoidance, adaptation and social comparisons) (26). Adaptations at home and in the nearby surroundings, as well as compensating with mobility aids and assistive devices, were strategies used to increase safety when performing daily activities and during ambulation. Other strategies were taking precautions, not being careless, and planning every action in advance in order to foresee a possible fall. The constant planning was a time-consuming activity, which reduced spontaneity and made participation in social events more difficult compared with their elderly non-disabled peers. However, when situations were perceived too challenging to perform many decided to avoid those activities or acted very carefully. In fact, this was often the case in activities related to ambulation when socializing with others. Similar strategies and solutions, such as organizing and planning activities, using assistive devices, adjusting the environment, or avoiding and accepting the situation, have been described in persons ageing with LEoP (27), in elderly persons (24), in persons with MS (19), stroke (17) and SCI (18). It is also important to consider these strategies in the rehabilitation of persons with LEoP, in order to reduce falls and fall-related consequences.
The findings of this qualitative study show that experiences of falls with regard to circumstances, possible causes, and consequences, as well as strategies to manage the impact of falls on daily life are complex. Therefore, falls and the consequences thereof should be carefully considered in the rehabilitation of persons with LEoP. A falls management programme targeting a variety of aspects should be developed. In addition to efforts to decrease physical impairments, prescribe mobility aids, housing adaptations and adjustments to the environment, it may also be important to improve the persons’ body awareness, self-efficacy, and knowledge of how to achieve balance between activity and rest, and to learn how to think strategically and plan actions in advance. Awareness of one’s capability and support to develop strategies to reduce falls may be helpful for these persons in order to increase overall functioning. A previous study (28) in persons with LEoP has described that an interdisciplinary rehabilitation programme can lead to a sense of increased control and life satisfaction. Future studies should therefore evaluate the effects of a multifaceted, interdisciplinary, goal-oriented falls management programme in persons with LEoP.
The 14 participants varied in terms of sex, age, disability and experiences of falls, and this diversity may have contributed to a broader understanding of how experiences of falls influence daily life. The sample size could be considered small, but is thought to be sufficient when the purpose is to describe shared perceptions (29). Trustworthiness was achieved in terms of credibility, confirmability and transferability (30). During data collection, a semi-structured interview guide was used, which helped the interviewers to cover the same areas in all interviews. The first and last authors had continuous discussions throughout the analysis and the findings were later scrutinized by the second author, which strengthened the credibility of the analysis. Concerning reflexivity, the authors made efforts to stay neutral in relation to the data; we strived for transparency throughout the data collection and data analysis, and the findings were presented with quotations. All authors were also aware that the results might be affected by their previous experiences as clinicians and researchers (20, 31). Qualitative interviews and systematic text condensations were found to be well-suited to the aim of the study. Only ambulatory persons with LEoP were included in the study, thus the results cannot be transferred to the entire population of persons with LEoP, but only to persons with the same level of disability.
In conclusion, experiences of falls greatly affect persons with LEoP in daily life. To reduce falls and fall-related consequences both problem-focused and emotion-focused strategies are used. In order to increase daily functioning these findings should be included in a multifaceted falls management programme.
The authors would like to thank all individuals who volunteered to participate in this study.
The study was supported by grants from Skåne county council’s research and development foundation, Stiftelsen för bistånd till rörelsehindrade i Skåne, Neuroförbundet, the Gyllenstierna Krapperup Foundation, the Norrbacka-Eugenia Foundation, the Department of Health Sciences, Lund University and the Faculty of Medicine at Lund
University, Lund, Sweden.
The authors declare no conflicts of interest.


 Click to show fullsize
Click to show fullsize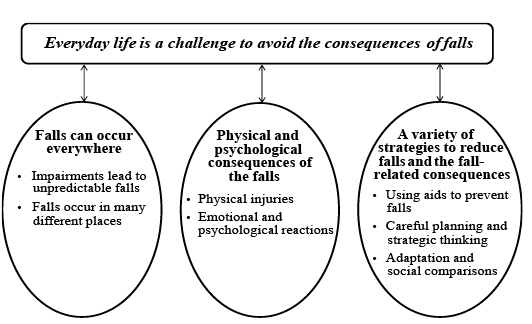 Click to show fullsize
Click to show fullsize